

AI: The Teammate Clinicians Need
Jay Rughani, Colin Rom, Olivia Webb, Will Shrank, and Vijay Pande
Our healthcare workers need our help.
Our clinicians are burned out. After the Covid-19 pandemic, only 57% of physicians said they would choose the field of medicine again. Another recent study reported nurse burnout rates higher than 50%.
Our clinicians are battling mental illness. Approximately 10% of physicians have reported having thoughts of suicide, and physicians have one of the highest rates of suicide of any profession.
Our clinicians are feeling less supported and it’s only getting worse. 25% of medical students in the US are considering dropping out.
The implications are devastating and will affect patient care. Health systems face growing staffing shortages, with 59% of clinicians believing their care teams are not adequately staffed. Over half of hospitals are already operating at a financial loss.
Given the burden we put on our healthcare workers, it’s perhaps no surprise that roughly one quarter of our nation’s $4.3 trillion in annual spending on healthcare can be characterized as “waste,” and that the largest source of that waste is administrative complexity. Our healthcare providers are being asked to do more with less: they are responsible for navigating complex billing and reimbursement systems, variable coverage schemes, and increasing documentation burden, all while taking greater responsibility for the proactive management of the health outcomes, quality of care, and patient experience of the populations for which they care.
This is not sustainable.
In many ways, the humane core of the profession is at risk. With so many requirements and distractions, the provider-patient relationship is less personal, more pressured, and far less satisfying for patients and providers than ever before.
How can we change this trajectory?
While it may seem ironic, AI solutions may be our best answer to the decaying personalization and humanity of care in the US; as Vijay wrote in 2021, “technology can make human healthcare more human.”
Our view is that 1) the latest advancements in AI offer a massive enablement opportunity to support our clinicians and 2) this can’t happen without the help of forward-thinking policymakers laying the payment infrastructure for AI-enabled care.
AI can make healthcare more human
By eliminating much of the mindless work and serving as an always-on copilot, AI tools can be an ever-present, always-ready teammate, freeing providers to spend their time on what matters most—communicating with and supporting the very personal needs and priorities of their patients.
To be clear—the goal in creating new AI tools is not to replace clinicians. It is to make them more successful, and to allow them to spend time on what matters: caring for patients.
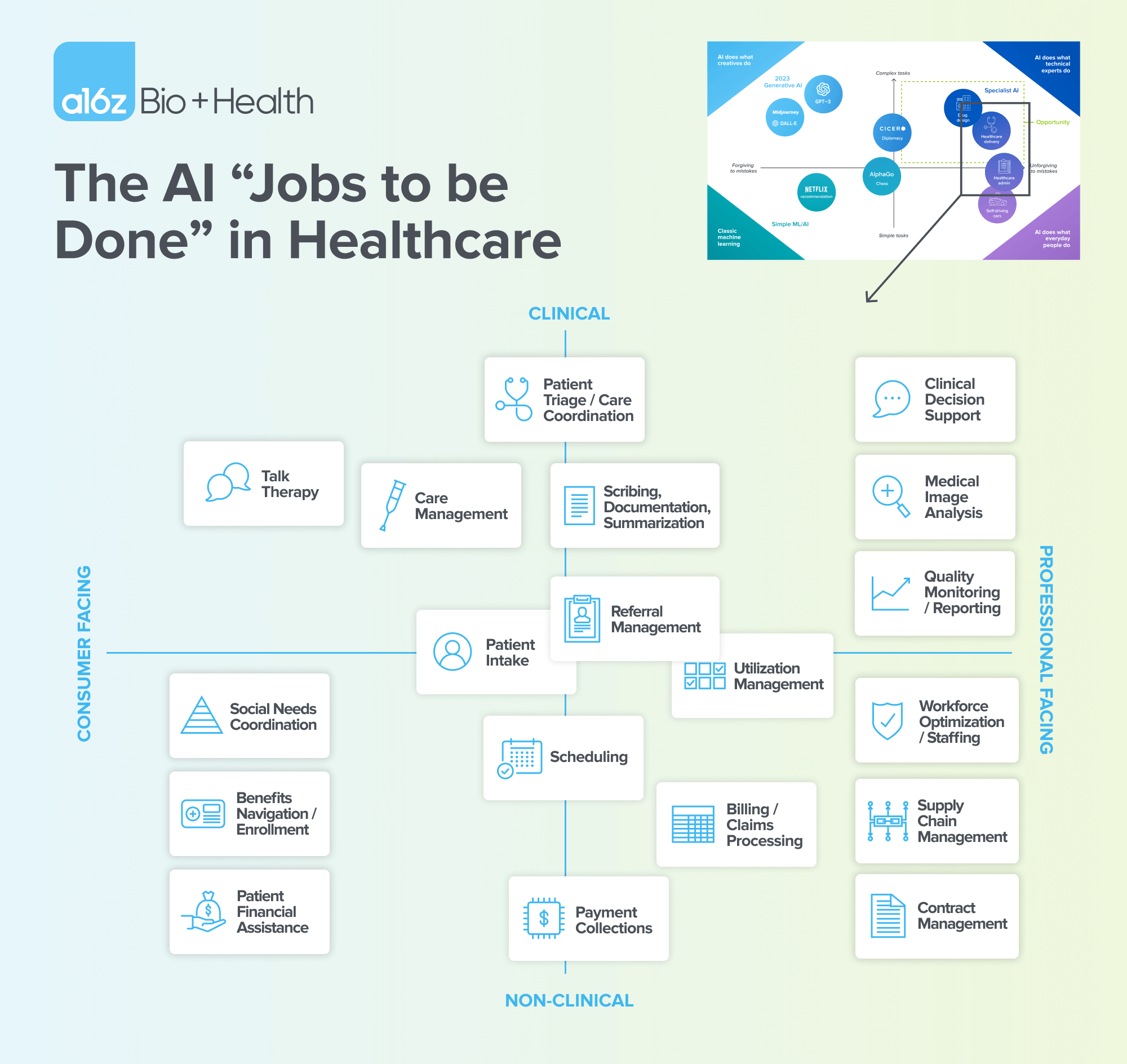
We recently wrote about the AI jobs to be done in healthcare and that building “specialist” AIs to perform healthcare tasks offers the greatest opportunity for impact. We believe that specially-trained AI models can drive wasteful spending away from clerical and administrative work and towards delivery of care. AI could accomplish this through expert patient triage, clinical decision support, image analysis, care management, and more.
The contours of the future are coming into focus. Technology is emerging for AI to augment and enable care. For example, a patient could present at a physician’s office and share symptoms with a nurse, who would “converse” about the symptoms with an infinitely knowledgeable and cheerful AI worker that could instantly risk-stratify the patient and predict the patient’s likelihood of experiencing an acute, time-sensitive event.
Once the patient is taken back to the clinician’s office, an AI physician’s assistant (PA) could listen in to the patient’s complaints as they share with the physician. That AI PA could automatically create a structured note allowing the human provider to focus on the patient during the visit, maintain eye contact and focus, and then review the note afterwards. The AI PA could also capture key documentation essential for coding and reimbursement, reducing the need for coding teams to assess the note and the back-and-forth with providers to optimize reimbursement.
Moreover, the AI PA could assist the physicians and nurses in diagnostics and treatment plan, by offering a thorough, evidence-based differential diagnosis and recommending best options for diagnostic testing that can pressure-test the clinician’s intuition. After the patient is treated, another AI PA could assist in identifying the most appropriate follow-up care for the patient, a task that, without AI, often requires manual and time-intensive phone calls.
For the patient, the AI PA could generate a report in plain English summarizing their diagnosis, treatment plan, and next steps, all using accessible language tailored to the patient’s situation.
In other words, the integration of AI into medical settings does not replace providers, it augments their abilities, allowing them to focus on the higher-order care that they’ve been trained to offer. Diagnostic ability, patient education, and bedside manner could take precedence over typing out medical records and managing billing processes.
From the patient perspective, this future isn’t one with automated, impersonal kiosks, but instead an experience that more closely resembles the ideal of one-on-one time with a trained, caring professional—concierge-level care at accessible prices.
The policy infrastructure for AI-enabled care
As this technology continues to improve, the policy infrastructure and evidence must as well. We waste approximately $1 trillion annually in the US healthcare system. As AI demonstrates the ability to do more human tasks at (orders of magnitude) lower cost, particularly healthcare-related tasks, it offers tremendous opportunities to lower that bill. Clinicians should be able to drive better results while keeping more of their revenue. The health system must test and learn, and policymakers and regulators have an opportunity to help facilitate that learning.
CMS has taken meaningful strides in supporting new care pathways with the implementation of Remote Patient Monitoring (RPM) and Remote Therapy Management (RTM) Codes. By creating a vehicle for providers to be reimbursed for delivering virtual and continuous care for specific conditions, CMS is designing a sustainable pathway for investment and development. CMS has signaled an interest in expanding coverage to more conditions.
To further drive uptake and access, CMS should take additional steps to implement reimbursement policies that recognize the costs associated with the utilization of AI-assisted/augmented care. For example, CMS could examine and update the direct cost inputs and indirect practice expenses to assure reimbursement reflects the rapid pace of innovation in AI, and the cost to practices adopting these technological breakthroughs. Moreover, CMMI could recommend and empirically study the impact of AI-enabling interventions within the context of an accountable payment model.
With appreciation of the fact that AI can improve economics for clinicians and reduce waste for taxpayers, we anticipate a considerable expansion of experimentation. And with that expansion will come better evidence to foster inclusion of these technological advances into value-based models, driving better care and better outcomes at lower costs.
Our providers need help, and the technology exists to help shoulder the burden. Through thoughtful policy shifts and patient-centric AI integration, our providers will be able to work alongside AI teammates providing the assistance they need.
-

Jay Rughani is an investing partner on the Bio + Health team at Andreessen Horowitz, focused on AI and data products across healthcare and life sciences.
-

Colin Rom is the public policy lead on the Bio + Health team, building CFI into a leading voice of health innovation in Washington, D.C.
- Follow
-

Olivia Webb is the editorial lead, healthcare, on the Bio + Health team.
-

Will Shrank is a venture partner on the CFI Bio + Health team.
-

Vijay Pande is the founding general partner of the Bio + Health team at Andreessen Horowitz, focused on the cross-section of biology and computer science.